Fully automated analysis
iDAScore is an AI-based scoring system that provides fully automated analysis of time-lapse sequences. Now you can get an objective ranking based on the likelihood of achieving a fetal heartbeat on days 2, 3 or blastocyst stage of each of a patient’s embryos at once – with just a touch of a button.
Learn more about iDAScore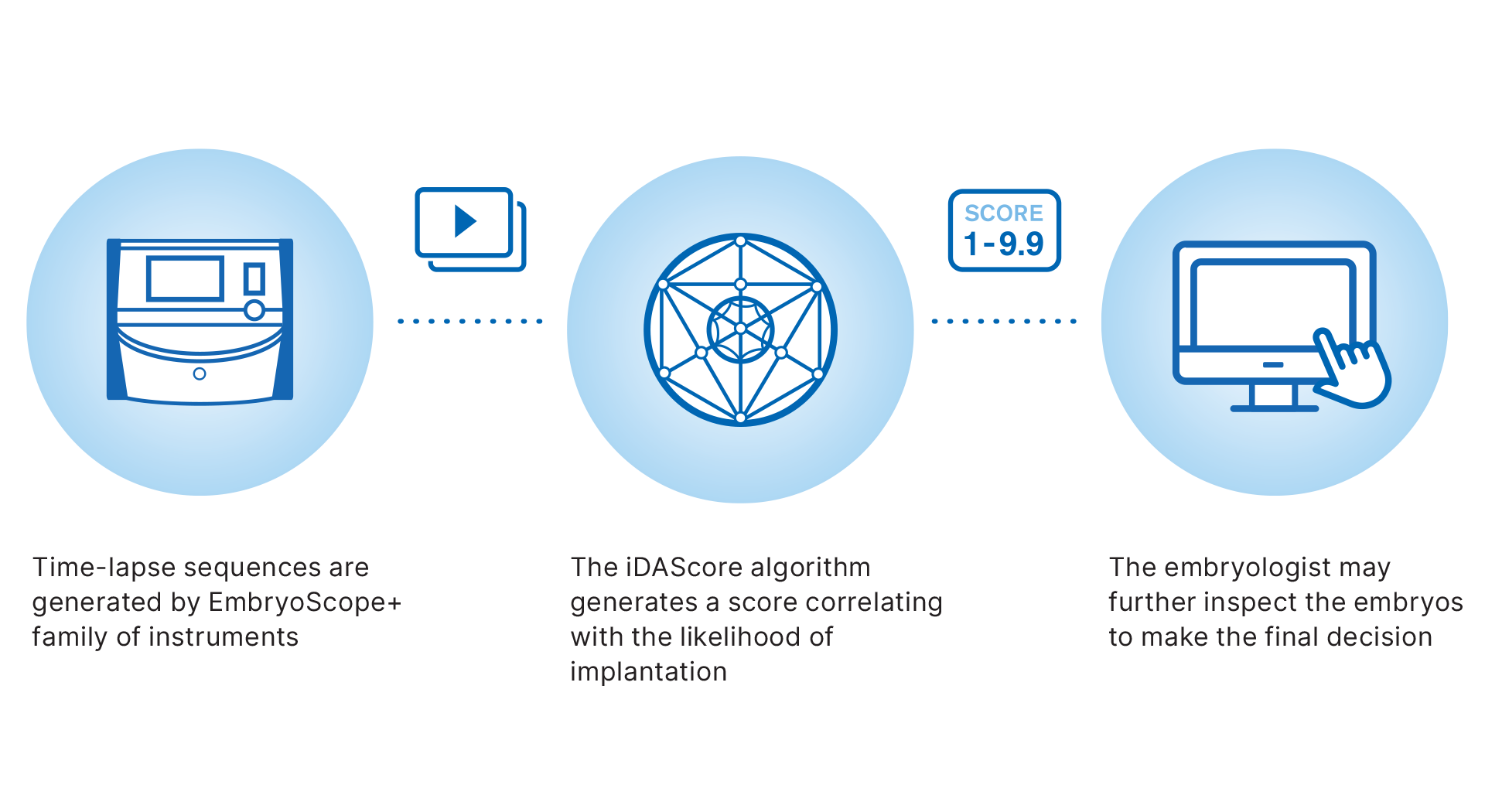
21.3+/- 18.1 seconds, compared to 208.3 +/-144.7 seconds using a standard manual assessment.
Illingworth et. al (2024), Nature Medicine, in press.


Watch the webinar:
The role of AI in improving clinical efficiency – Results from the first RCT for AI based selection
In this presentation, Dr Peter Illingworth (Virtus Health) present the results of the world-first randomised controlled trial (RCT) evaluating the use of deep-learning AI for embryo selection in IVF. Following this, Jørgen Berntsen (Vitrolife Group) delve into the development and background of the second version of this innovative technology. Finally, David Gardner (Virtus Health) discuss the significant benefits this technology brings to the IVF laboratory, including enhanced consistency, efficiency, and objectivity.
This webinar was held September 2024.
Watch webinar
Reflections from the authors on the study
Together with the other clinic collaborators we’re very proud to be the first in the world to carry out a randomised trial to evaluate the embryo selection ability of a deep-learning AI compared to an embryologist manually assessing them, based on physical appearance.
There is no doubt this study has huge significance, as we have witnessed first-hand at our clinics how it has improved the way we work.
- Dr Peter Illingworth, Virtus Health
Our world-first trial demonstrates that blastocyst selection using deep-learning AI can not only attain similar pregnancy rates to using the Gardner grade, but it dramatically reduces the time associated with the process.
- Prof David Gardner, Virtus Health
These findings signify a pivotal moment in our field, as AI-powered embryo selection paired with time-lapse incubation shows its potential to achieve success rates on par with conventional methods, while notably reducing the time required for this critical task.
- Dr Aishling Ahlström, Livio, Sweden
This not only benefits patients by standardising embryo selection and potentially shortening the time to achieve a pregnancy but also optimises the use of resources in IVF clinics.
- Dr Christos Venetis, IVF Australia, Virtus Health
By integrating AI with time-lapse technology, this sets a new standard for consistency and efficiency in embryo selection.
- Prof Scott Nelson, University of Glasgow, UK
This study shows that deep-learning AI can be used to optimise clinical resources by saving time spent on evaluating embryos without compromising clinical outcomes. It is an exciting time for innovation within the field of IVF, which is exemplified by the fact that the version of iDAScore used in the study has already been improved.
- Jorgen Berntsen, Data Science Manager, Vitrolife
Building on the power of AI
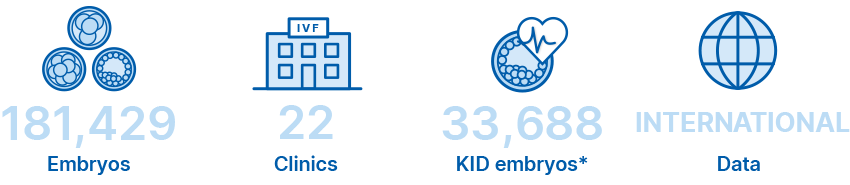
The iDAScore algorithm was developed by our own AI team and trained on full time-lapse sequences of now more than 180,000 time-lapse sequences of embryos with known clinical fate.
Diverse data to minimise bias
Data diversity and size can reduce bias in AI-based embryo selection by providing the model with a more representative sample of the population it will be used on. Diversity in the dataset means that the model is exposed to a wide variety of input patterns, which allows it to learn from a broad range of examples such as patient profile and clinical protocols. This can help to prevent the model from becoming overly specialised to a specific subset of the population, wich can lead to bias.
The iDAScore input is comprised of a wide variety of data that have been collected across three continents.The data represents a wide variety of patient profile and clinical practices including oocyte origin, IVF and ICSI, clinical protocols, and patients’ age. It includes data from both fresh and frozen embryos with known outcome.

57% more data on embryos
iDAScore has been further trained on data from an additional 65,000 embryo time-lapse sequences. iDAScore now includes embryo ranking on day 2 and day 3 in addition to blastocyst evaluation.
Performance of iDAScore
iDAScore has been validated to correlate with clinical outcomes including implantation and live birth.
Live birth rate increases by iDAScore group in all age groups3
Live Birth stratified by age of 3010 Single Vitrified Blastocyst transfers
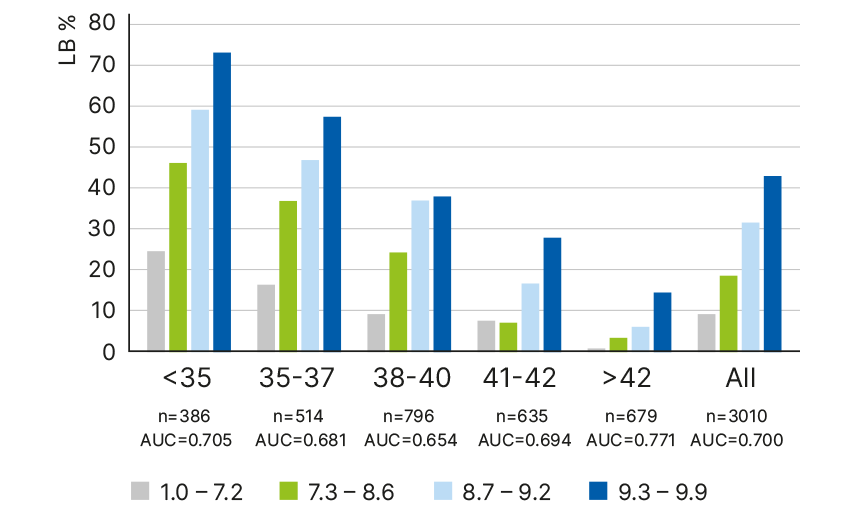
OR Live Birth 1.811 95% C.I. 1.666-1.976 p<0.05.
Multivariate adjusted OR 1.535 95%CI 1.358-1.736, p<0.05. P <0.05. for all age groups. OR = 1,811 (1.666-1.976).
aOR = 1.535 (1.358–1.736). n= # transfers in each age group.
The higher the iDAScore the higher the likelihood of implantation4
Implantation rate
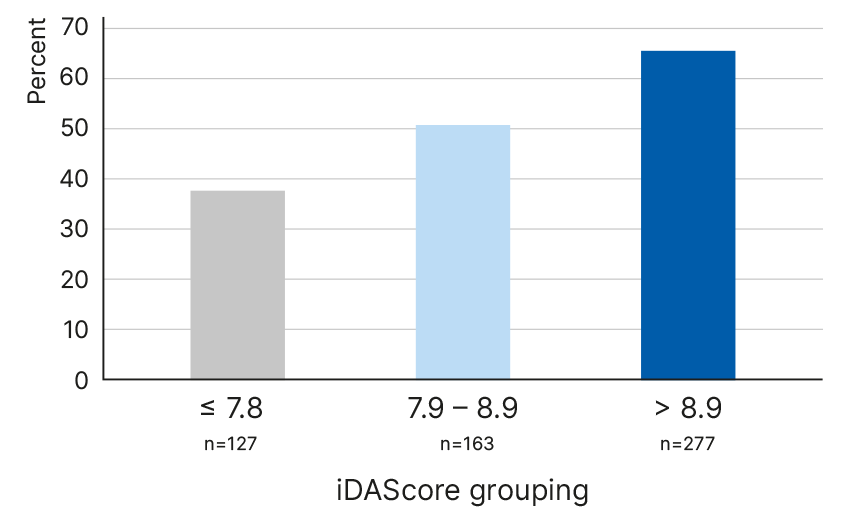
OR Oocyte donor 1.61 1.19-2.19 p<0.001
OR autologoous 1.52 1.22-1.90 p<0.001
Our findings confirm that embryo evaluation can be performed automatically allowing embryologists to utilise their time more efficiently in other tasks of the IVF process that are more complex and require high precision and attention.
Explainability AI
Rather than assigning weight to any individual event, all development events are taken into consideration in the context of the entire development sequence. Although iDAScore does not specifically use any particular parameters to generate a score, it correlates well with known features of embryo development linked to viability.
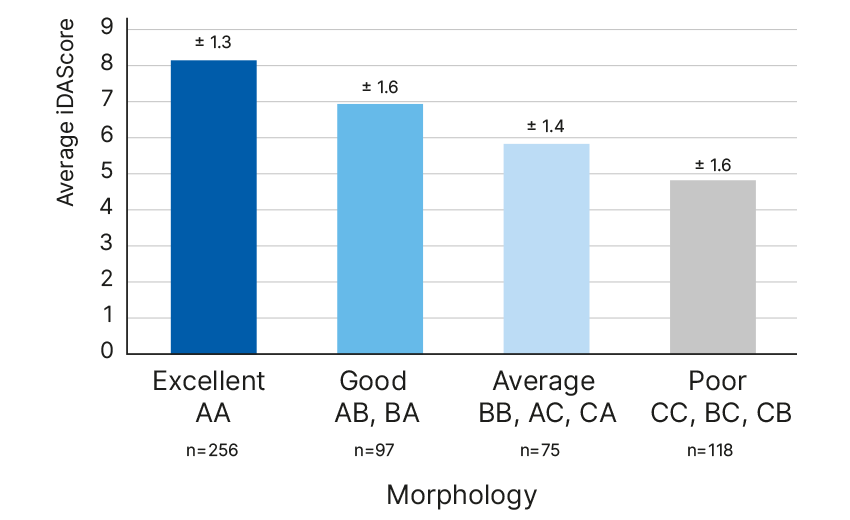
iDAScore correlation with embryologist’ gradings5
Association between iDAScore v1.0, senior embryologists’ grading
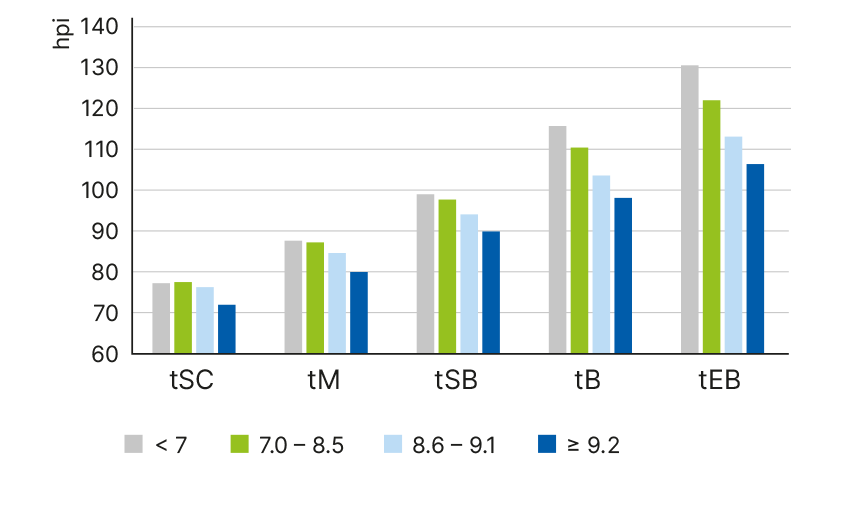
iDAScore is related to pace of development6
iDAScore group and development pace
Blastocyst with higher iDAScore have fewer cell exclusions7
Percentage blastocysts with cells excluded before compaction
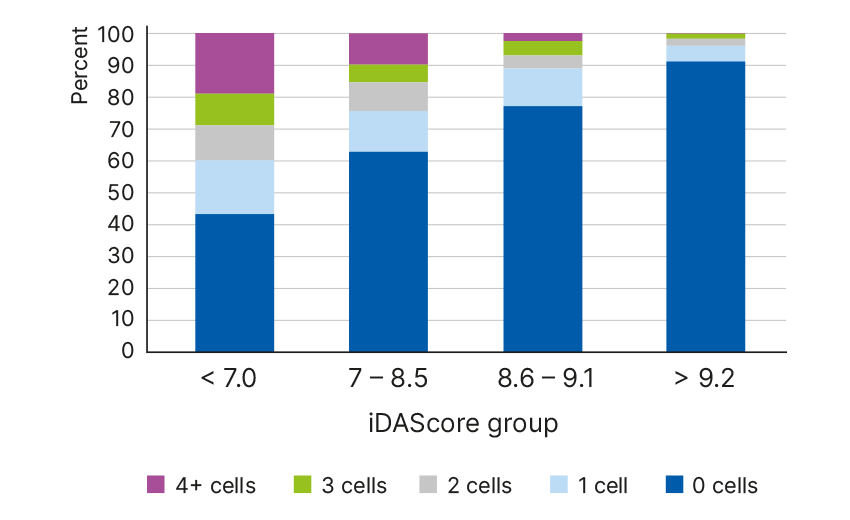
n=1503 blastocysts analysed
p<0.0001 for each morphokinetic interval
iDAScore is related to direct cleavages7
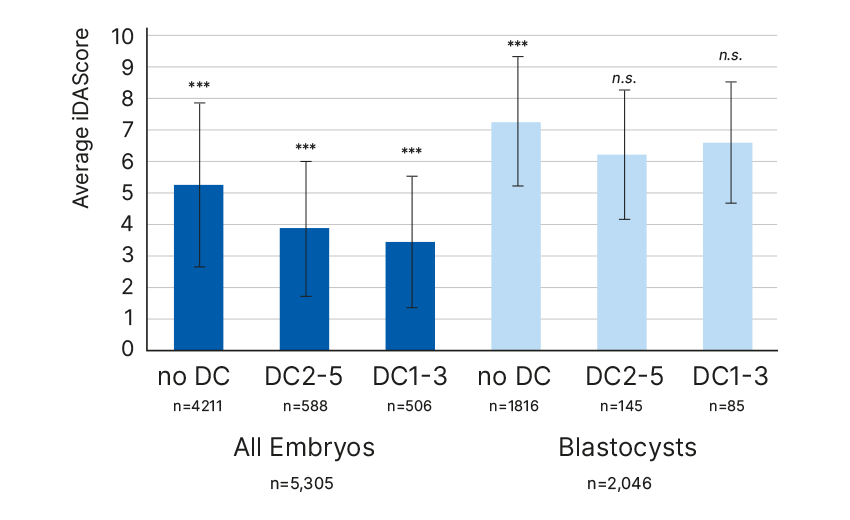
DC1-3: t3-tPNf < 5 hours, DC2-5: t5-t3 < 5 hours
“iDAScore does not require any manual, user-dependent annotations, enabling objective assessment of embryos that are cultured to the blastocyst stage. Therefore, iDAScore is an optimal method for scoring embryos and prioritising blasto- cysts for transfer without compromising live birth and neonatal outcomes.” 3
“Our findings confirm that embryo evaluation can be performed automatically allowing embryologists to utilise their time more efficiently in other tasks of the IVF process that are more complex and require high precision and attention.” 4
"With just a touch of a button, it provides us with scores instantly. It is impressive and this helps us improve our workflow and efficiency dramatically as there will be no need for annotations. It is a great tool for improving consistency in our evaluations as well.”
-Hana Watanabe, Embryologist, Hiroshima HART Clinic, Japan

“With a clear easy to use interface iDAScore makes choosing between multiple blastocysts an easier job. The score matches well with the decisions of experienced embryologists, and KIDScore D5. We think that in time, iDAScore will become an invaluable tool in helping to make our day to day clinical decisions. In addition, we are hoping to use it to assess already frozen embryos which were cultured in the EmbryoScope+. ”
-Alan Birks, Senior Clinical Embryologist
Manchester Fertility, UK

"iDAScore provides an impressive ranking of embryos. We see that the correlation with implantation, shows the same positive trend as with the KIDScore D5 decision support tool. This could be a game changer in the future of embryo evaluation, as we gain more trust in using AI for embryo evaluation.”
-Tony Price, Embryology Manager
Wessex Fertility, UK

“iDAScore is an ideal tool for providing a fast prioritization of embryos for further examination. This is especially useful for guiding new embryologists and helping them to evaluate embryos in a way that is more consistent with evaluation by senior staff with many years of experience.”
-Kirsten Simonson, Clinical embryologist
Maigaard fertility, Denmark

Explore the latest publications about iDAScore®
In this summary, we have curated the latest science publications and selected abstracts about iDAScore for your easy access. Discover articles that cover topics such as deep learning for embryo selection across multiple transfer days, validations, comparison of performances and much more.
Stay up to date - download nowA complete solution with the world’s leading time-lapse systems
Vitrolife has everything your clinic needs to maximise time-lapse culture and evaluation. Whether you want to implement and enjoy the benefits of an integrated time-lapse system for 8, 15 or 24 patients or complement your current set-up with more time-lapse incubation capacity.
* Not FDA510(k)-cleared and not available for sale in the United States of America.

 8 culture dish positions per incubator
8 culture dish positions per incubator

 24 culture dish positions per incubator
24 culture dish positions per incubator
Watch the webinar:
Embryo Evaluation's Latest Software Release: Find out what's new
Are you looking to stay up to date with the latest advancements in embryo evaluation software? Watch this short webinar, where we'll showcase the update of the iDAScore® software and its features.
Watch nowGet in touch
Don't hesitate to contact us or your sales rep if you have any questions or want more information about iDAScore.
Contact usReferences
1. Bormann et. al (2020), Fertil Steril 113(4): 781-787.e1.
2. Storr et. al (2017), Hum Reprod 32(2): 307-314.
3. Ueno et al. (2022), JARG (39) 2089-2099.
4. Bori et al. (2022), Human Reproduction 37(Suppl.1).
5. Casciani et al. (2022), Human Reproduction 37(Suppl. 1).
6. Ezoe et al. (2022), Reprod Biomed Online 45(6):1124-1132.
7. Berntsen et al. (2022), PLoS ONE 17(2): e0262661.